

To the Editor,
Aneurysms and pseudoaneurysms develop in approximately 8% of arteriovenous fistulas (AVF) created for haemodialysis.1 They are potential sources of embolisation and thrombosis, and can occasionally erode the skin, giving rise to infection and local bleeding, and can even deform the affected limb. True aneurysms in AVF are dilations in which the structure of the vein or artery wall remains intact. They frequently consist of venous aneurysms in long-term autologous fistulas associated with venous stenosis. True arterial aneurysms are less common and frequently occur in the axillary or humeral arteries following ligation of an AVF in the elbow.1 The increase in arterial flow and wall vibration are believed to be involved in the pathogenesis of this condition. On the other hand, pseudoaneurysms or fake aneurysms are expandable dilations caused by persistent subcutaneous bleeding through a continuous deterioration of the fistula or prosthesis wall.2
CLINICAL CASE
A 65 year-old male was referred from the nephrology department to the vascular surgery unit due to a large pulsatile mass in the left forearm that has been present for several years, undergoing an accelerated and progressive growth in recent months. The patient had a background of arterial hypertension, dyslipidaemia, and a left radiocephalic fistula created 20 years earlier for haemodialysis due to terminal chronic renal failure. Six years after having received a transplant, this fistula was ligated.
The physical examination revealed an enormous pulsatile mass in the anterior side of the left forearm, with no signs of thrill or murmur (Figure 1). The hands were well perfused, with both radial and ulnar pulses present.
We first performed a Doppler ultrasound analysis, which revealed intense blood flow within the mass, although we were unable to determine whether this was an aneurysm or pseudoaneurysm. We proceeded with an axial computed angiotomography angiography (CTA), and we were able to observe an enlarged and elongated humeral artery, an aneurysm or pseudoaneurysm of 62 millimetres in diameter in the radial area, permeable ulnar and interosseous arteries, and an obstructed distal radial artery.
The suspected diagnosis of aneurysm or pseudoaneurysm of the radial artery secondary to a ligated radiocephalic AVF in the transplant recipient led to the indication of surgical treatment.
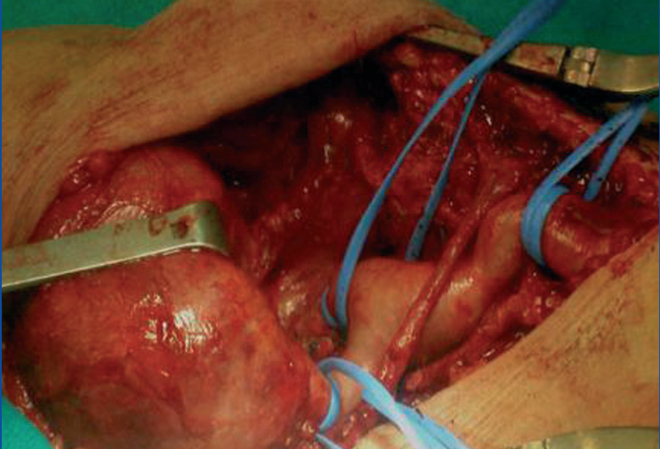
We performed incisions in the elbow joint and distally along the radius, and then isolated the humeral, radial, and ulnar arteries, observing a giant true aneurysm along the entire radial artery. We completely resected the aneurysm and performed a proximal and distal ligation of the radial artery, since it was chronically thrombosed (Figure 2) and the vascularisation of the hand was ensured by the continuity of the ulnar and interosseous arteries.
The postoperative period went without incident. Upon discharge, the patient’s humeral and ulnar pulses were constant, with good perfusion in the hand. A histological analysis confirmed that this was indeed a true aneurysm of the radial artery. One year following treatment, the patient is asymptomatic and without complications.
DISCUSSION
True arterial aneurysms in the peripheral arteries are rare, and only 5% of them are located in the arms. They are most commonly associated with local traumas and systemic diseases (atherosclerosis, giant cell arteritis, and fibromuscular dysplasia).2 The scarcity of this pathology makes it difficult to evaluate its epidemiological and clinical characteristics. In AVF created for haemodialysis, sporadic cases of true arterial aneurysms have been described, primarily in the axillary or humeral arteries and following ligation of an AVF in the elbow after kidney transplantation.3 In transplant recipients with well-functioning grafts after a reasonable period of time, ligation of an AVF for haemodialysis is a controversial procedure. However, it is usually performed in order to avoid complications such as oedema, vascular access steal syndrome, high cardiac output, thrombosis, venous aneurysms, pseudoaneurysms, bleeding, and aesthetic defects.1,4
The diagnosis of aneurysms and pseudoaneurysms tends to be clinical, in the presence of a pulsating mass with progressive growth in the area of the vascular access. Pulses distal to the lesion may or may not be present.5 A Doppler ultrasound may reveal flow in the aneurysmal sac, thrombosis, or haematoma. In unclear cases, a CTA scan or magnetic resonance can be useful. Fistulography may be indicated if the aforementioned techniques do not provide sufficient information,1 and can be especially useful for planning surgical treatment.
True arterial aneurysms must be quickly treated due to the risk of local and systemic complications, including embolisation, thrombosis, skin erosion and infection, bleeding, and compression of adjacent nervous structures, producing paraesthesia, pain, and reduced mobility.6 The treatment of choice is a resection of the aneurysm and arterial reconstruction4 in order to guarantee adequate perfusion of the limb after the aneurysm has been excluded from circulation. Another option is endovascular treatment.7 In our case, we opted for resection and ligation of the radial artery, since it was chronically obstructed and the perfusion of the hand was guaranteed by the ulnar and interosseous arteries.
Venous aneurysms do not require treatment unless they are associated with severe stenosis, necrosis, or skin disorders and there is a risk of rupture of the aneurysm. Severe stenosis can be treated with angioplasty. If necrosis or the risk of aneurysmal rupture appears, a surgical review is necessary.2
Pseudoaneurysms are ruptures contained by the soft tissue that occur primarily in puncture sites. Pseudoaneurysms of PTFE (polytetrafluoroethylene) prostheses can also be treated using percutaneous or surgical approaches.1 In the absence of infection, a local repair can ensue by suturing the graft defect or by graft interposition.1,8 To conclude, we would like to point out that aneurysmal dilations are complications that can jeopardise both the viability of the vascular access and the life of the patient. As such, it is essential to make a correct differential diagnosis between aneurysms (arterial and venous) and pseudoaneurysms for proper treatment planning, since the appropriate treatment varies with each case.
Conflicts of interest
The authors affirm that they have no conflicts of interest related to the content of this article.

Figure 1. Physical examination

Figure 2. Surgical treatment



