

Introducción: La insuficiencia renal crónica (IRC) constituye un factor de riesgo cardiovascular independiente. El conocimiento de su prevalencia en la población general puede contribuir a la detección precoz de esta enfermedad y de prevenir o retrasar su evolución. Métodos: Se seleccionó una muestra aleatoria de población general española, con edad igual o superior a 20 años, distribuida por todo el territorio nacional y estratificada por hábitat, edad y sexo conforme al censo de 2001 (n = 2.746). Se recopilaron datos sociodemográficos y clínicos, y se evaluó la prevalencia de IRC mediante determinación centralizada de creatinina sérica y aplicación de la ecuación MDRD. Se llevaron a cabo análisis univariantes y multivariantes para evaluar la asociación entre la IRC y diversos factores de riesgo. Resultados: La edad media fue de 49,5 años. La prevalencia global de IRC en estadios 3-5, según la Kidney Disease Outcomes Quality Initiative, fue del 6,8%, con un intervalo de confianza del 95% (IC) de 5,4 a 8,2 (3,3% para edades 40-64 años y 21,4% para edades >64 años). Las prevalencias estimadas para cada uno de los estadios de IRC fueron: 0,99% para estadio 1 (tasa de filtrado glomerular [TFG] >_90 ml/min por 1,73 m2 con proteinuria); 1,3% para estadio 2 (TFG 60-89); 5,4% para estadio 3a (TFG 45-59); 1,1% para estadio 3b (TFG 30-44); 0,27% para estadio 4 (TFG 15-29), y 0,03% para estadio 5 (TFG <15). Se apreció una prevalencia considerable de factores de riesgo cardiovascular clásicos: dislipemia (29,3%), obesidad (26,1%), hipertensión (24,1%), diabetes (9,2%) y tabaquismo activo (25,5%). Los factores predictores independientes de IRC fueron la edad, la obesidad y la hipertensión previamente diagnosticada. Conclusiones: La prevalencia de IRC (en cualquier estadio) en la población general española es relativamente elevada, en especial en los individuos de edad avanzada, y similar a la de otros países del mismo entorno geográfico. Además de la edad, dos factores de riesgo modificables, la hipertensión y la obesidad, se asociaron con una mayor prevalencia de IRC.
Introduction: Chronic kidney disease (CKD) is an independent cardiovascular risk factor. The knowledge of prevalence in general population may help to early detection of CKD and prevent or delay its progression. Methods: Sociodemographic, baseline characteristics, and CKD prevalence (measured by centralized serum creatinine and MDRD equation) were evaluated in a randomly selected sample of general population aged 20 years or older, collected in all Spanish regions and stratified by habitat, age and sex according to 2001 census (n = 2,746). Univariate and multivariate logistic regression analyses were used to evaluate associations with CKD risk factors. Results: Mean age was 49.5 years. The overall prevalence of Kidney Disease Outcomes Quality Initiative grades 3-5 CKD was 6.8%, with a 95% confidence interval (CI) of 5.4 to 8.2 (3.3% for age 40-64 years and 21.4% for age >64 years). The prevalence estimates of CKD stages were: 0.99% for stage 1 (glomerular filtration rate [GFR] >_90 ml/min per 1.73 m2 with proteinuria); 1.3% for stage 2 (GFR 60-89); 5.4% for stage 3a (GFR 45-59); 1.1% for stage 3b (GFR 30-44); 0.27% for stage 4 (GFR 15-29); and 0.03% for stage 5 (GFR <15). An important prevalence of classical cardiovascular risk factors was observed: dyslipemia (29.3%), obesity (26.1%), hypertension (24.1%), diabetes (9.2%) and current smoking (25.5%). The independent predictor factors for CKD were age, obesity and previously diagnosed hypertension. Conclusions: The prevalence of CKD at any stage in general population from Spain is relatively high, especially in the elderly, and similar to countries of the same geographical area. Independently of age, two modifiable risks factors, hypertension and obesity, are associated with an increased prevalence of CKD.
.

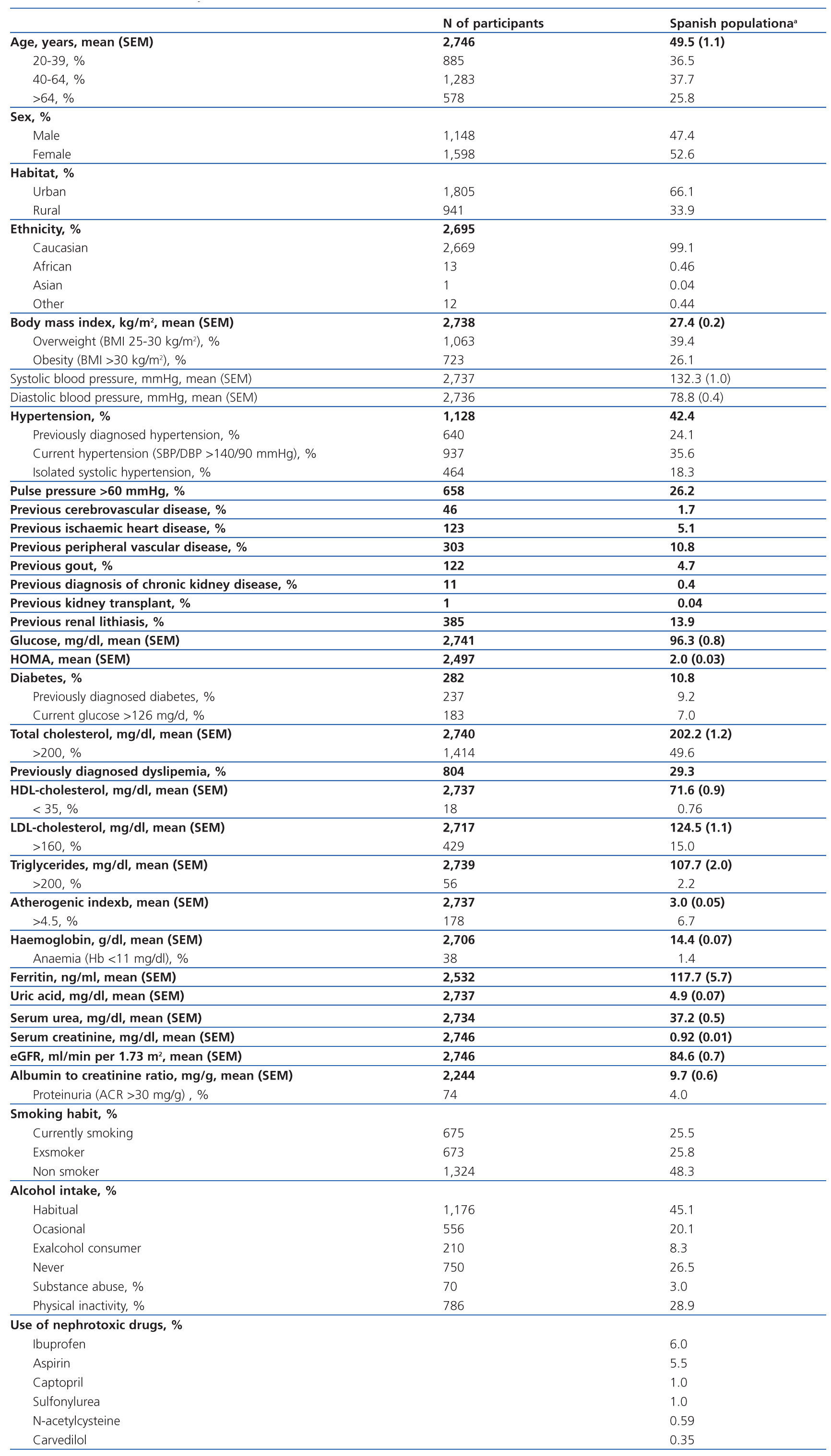
Tabla 1. Demographic and clinical characteristics of Spanish population aged 20 years or older based on the cohort collected in the EPIRCE study (n = 2,746).

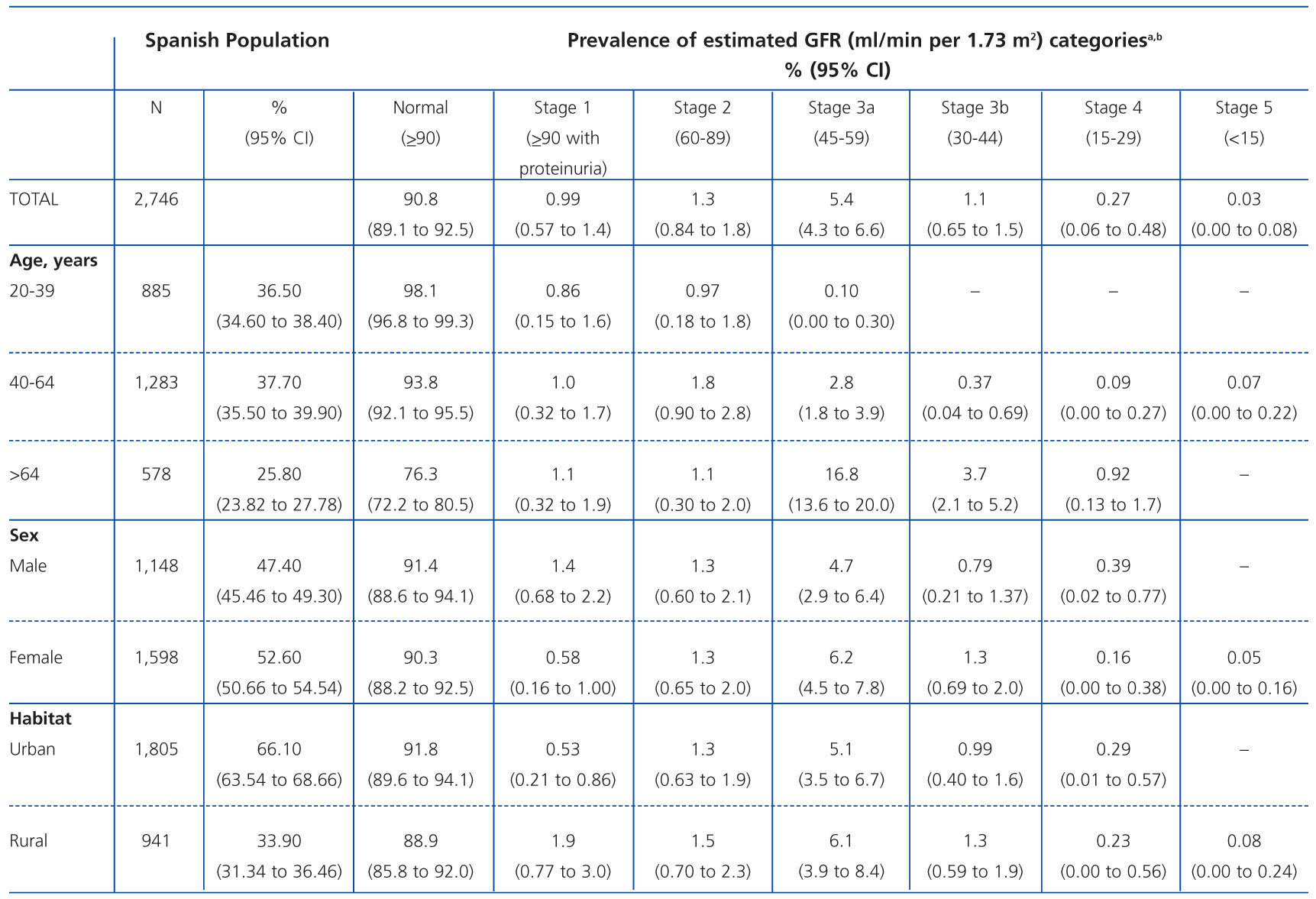
Tabla 2. Prevalence of chronic kidney disease in the Spanish population aged 20 years or older based on thee cohort collected in the EPIRCE study (n = 2,746).

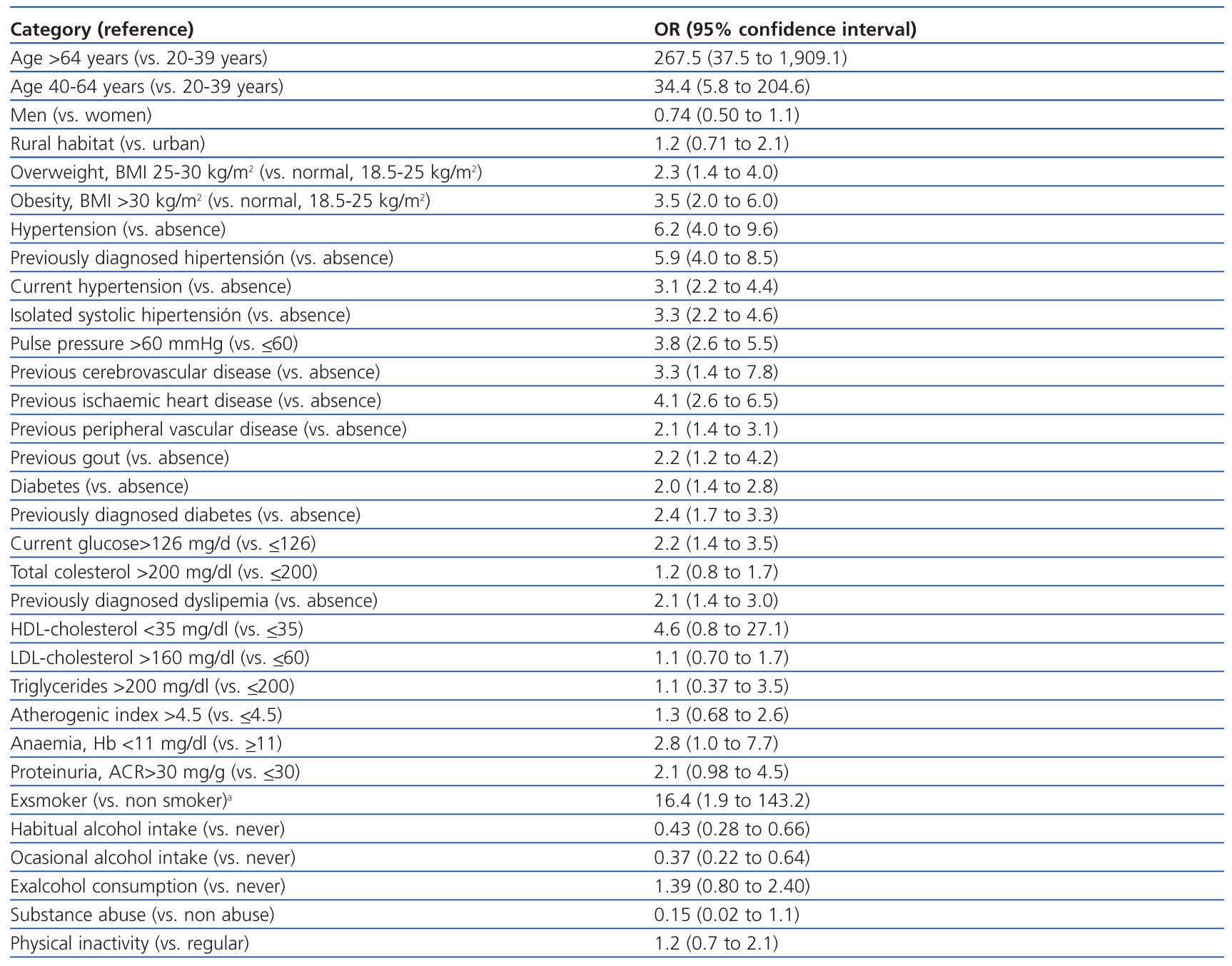
Tabla 3. Unadjusted associations between demographic or clinical characteristics and the presence of chronic kidney disease (eGFR <60 ml min per 1 73 m2

Tabla 4. Independent predictors of chronic kidney disease (eGFR <60 ml min per 1 73 m2 in the multivariate logistic regression model



