
The severity of the disease and the evolution of patients infected with the type 2 coronavirus that causes severe acute respiratory syndrome (SARS-CoV-2) has been associated with advanced age, comorbidities such as obesity, hypertension, diabetes, and chronic kidney disease.1–8 The Spanish Society of Nephrology (SEN), the Spanish Society of Transplantation (SET) and the National Transplant Organization (ONT) have published protocols and recommendations aiming to prevent the infection of kidney patients8–12 and professionals involved in their care.12 Since the beginning of the first large epidemiological wave, we insisted on general and specific rules for protection (extensive information to patients, reasonable limitation of collective transport, systematic interviews to patients before each hemodialysis session, telematic visits that whenever possible, etc.). Since the initial days of pandemic there was a remarkable initiative to promote a registry of cases of renal patients that has allowed us to be informed weekly about the situation of the disease and provide clinical evidences that are highly relevant.13–18
COVID-19 in kidney transplant patientsSince the first months of the pandemic, numerous publications of clinical cases, case series, and registries have described the clinical features of COVID-19 in kidney transplantation (KT).13–30 The incidence and mortality rate are higher than in the general population and it was found that the poor prognosis was associated to similar variables as in the general population, such as advanced age or severe pneumonia. As in the general population, no specific treatment has been shown to be effective, and only general and respiratory support are truly relevant in the therapeutic strategy. The potential benefit of high-dose steroids30 has not yet been confirmed in renal patients.
Safety of kidney transplantsDuring the months of March and April 2020, due to the collapse of the intensive care units and the almost exclusive dedication to the care of patients with COVID-19, most organ donation and transplant programs reduced their activity, or even were suspended. Thereafter, the activity progressively recovered, and expert professionals have adapted the programs to the new reality.31–34 One of the most important concerns of professionals responsible of kidney transplant (KT) programs the need for a safe KT given the indisputable evidence that there are alternative renal replacement treatment techniques, such as peritoneal dialysis and hemodialysis, that allow transplantation to be deferred and done in maximum safety conditions. The fact that RT is the most favorable option of RRT with the best rehabilitation and greater survival34 may not justify the risk of reducing safety of the procedure, in an epidemiological pandemic scenario (Table 1).
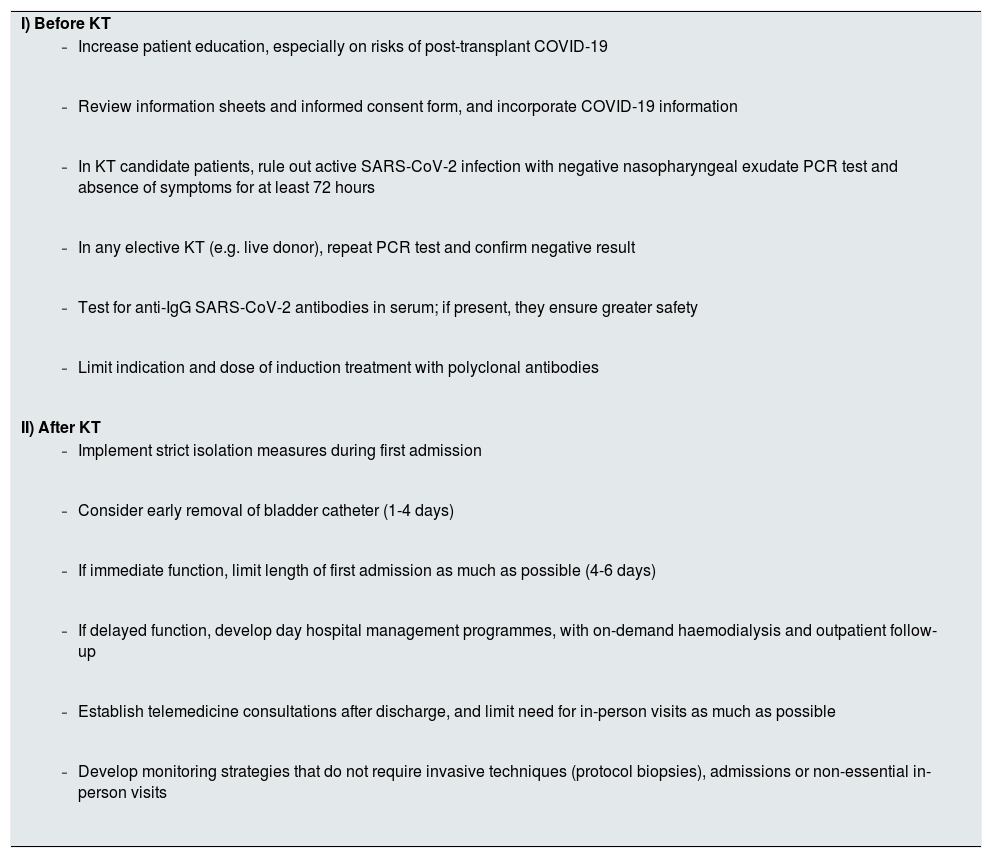
Recommendations for safe kidney transplantation (KT) during the COVID-19 pandemic.
| I) Before KT |
|
|
|
|
|
|
| II) After KT |
|
|
|
|
|
|
As recommended by ONT to guarantee the protection of patients on the waiting list, patients will undergo an exhaustive medical history inquiring about contact with suspected or confirmed cases, or if there is any symptoms compatible with COVID-19.11 SARS-CoV-2 screening should be performed by RT-PCR in a respiratory tract sample before the procedure of renal implant, antigen testing or virus serology being discouraged as an alternative to RT-PCR for screening. The transplant will not be performed until the result of the PCR is available. At this moment, there is no evidence to recommend the systematic performance of chest CT as a screening test in patients without clinical data suggestive of active infection.
Evidently, to avoid aggravation of the infection, if a patient on the KT waiting list is a suspected or confirmed case of COVID-19, he will be excluded from the list and will remain a temporary contraindication for KT until complete cure occurs. This will be established after a minimum period of 14 days since the onset of symptoms, with at least three days free of symptoms and a negative CRP; at this point the patient can be included in kidney transplant list.
In this sense, the ONT also recommends the review of informed consents for transplantation, including relevant information about the COVID-19 infection as part of the general process of information to the potential recipient or their legal representative.11
Based on data from the SEN COVID-19 registry, we have reported a special risk of severe COVID-19 and high mortality in recent KT recipients.16,17 Therefore, strategies should be developed whereby the hospital admission time is as short as possible, including intensive telematic monitoring, management strategies as outpatient in hospital facilities with SARS-CoV-2 free circuits, and very early diagnosis of any symptoms potentially related with COVID-19.32–35 The development of non-invasive monitoring tools, that were already relevant, now become essential; and of course, quality research and development in this area should be a priority.35
Kidney transplant after a COVID-19 episodeThere is little published evidence about the safety of KT in patients who have survived a mild36 or asymptomatic37 episode of COVID-19. In this issue of the journal, two very interesting experiences are being reported, in which the authors describe the cases of three patients who received a KT after having overcome the disease.38,39
The two cases reported from India are unique and constitute original contributions.38 It is the first patient reported to undergo a transplant after overcoming COVID-19 pneumonia (four weeks after the initial diagnosis), and the first recipient of a kidney from living donor in which both donor and recipient simultaneously presented previous mild symptomatic COVID-19. In both cases, the recipients were negative at the time of renal implantation and presented anti-SARS-CoV-2 IgG antibodies.
The case from Spain39 is the first case reported of advanced age (70 years). On this occasion, COVID-19 was found when the patient did not present symptoms, as a screening immediately prior to a KT from a deceased donor. After several positive PCR tests, alternating with some negative ones, it was decided to put him back on the list and he was transplanted with a negative PCR that was repeated frequently after transplantation. Although the authors acknowledge that there is no supporting evidence, they decided to confirm negativity to the virus with three consecutive PCR tests. It is possible that the specific characteristics of kidney patients, especially those who undergo periodic dialysis treatment, make it advisable to wait at least four weeks after a negative PCR, before proceeding with intense immunosuppression of a KT. In addition, it must not be forgotten that the sensitivity of PCR does not exceed 75–80%, and therefore it is advisable its repetition on at least two to three consecutive occasions. Besides certainty in the negativity of the PCR, it seems pertinent to verify the existence of sufficient titers of anti-SARS-CoV-2 IgG antibodies while the patient is awaiting for a KT. In this patient the disappearance of IgG antibodies was verified after having demonstrated their presence. It seems reasonable to think that the disappearance of IgG antibodies does not contraindicate KT, but with the current state of our knowledge, the documentation of each case should be as exhaustive as possible. This experience reinforces the concept that a past COVID-19 episode does not guarantee adequate long term protection, and in no way should preventive measures against possible infection should be relaxed.
Given the high incidence of COVID-19 in dialysis patients, it is very likely that throughout the world, patients with a past COVID-19 infection are being transplanted, especially in countries with very high transplantation activity as in Spain. It is necessary to collect experiences in this regard and to know the evolution with detail, learn whether respiratory or other sequelae are detected, if IgG antibodies are preserved over time and if reinfections occur.40 Transplant teams must be most careful in the analysis and orderly follow-up of these cases.
Conflict of interestThe authors declare that they have no conflict of interest.
Please cite this article as: Pascual J. Trasplante renal después de una COVID-19. Nefrologia. 2021;41:91–94.



