
The aim of this study was to share our experience and add further evidence to those studies already published in the literature proposing haemodialysis (HD) with high-cut-off (HCO) dialysers as a promising option in the treatment of myeloma kidney.
We conducted a prospective study from November 2012 to February 2015 and evaluated eight patients with multiple myeloma and acute renal failure requiring dialysis, with serum free light chain (FLC) levels >500mg/L (measured by nephelometry; FREELITE®, The Binding Site, Birmingham, United Kingdom).
All patients received treatment with bortezomib-based regimens.
The patients signed a consent form after being informed about the technique.
Two patients had renal biopsy, with a histopathology diagnosis of cast nephropathy. Renal biopsy was not performed in the remaining cases because of hemathologic abnormalities.
The patients had a 8-h HD sessions with a HCO 2100 dialyser (Theralite®, 2.1m2, Gambro, Deerfield, Illinois, USA), using the HD monitors routinely used in our unit (5008 CorDiax®, Fresenius Medical Care, Bad Homburg, Germany), with blood flows of 250–300mL/min and ultrapure dialysis fluid flow of 500mL/min.
Heparinisation was achieved with hourly doses of unfractionated sodium heparin (initial dose of 0.5mg/kg in the first hour and 10mg/h with adjustment according to aPTT after 4h).
Replacement fluid after each session was albumin 20% (100mL), monosodium phosphate (10mL), 1M magnesium sulphate (10mL) and calcium gluconate. These supplements were adjusted according to the needs of each patient.
The treatment regimen included 5 sessions in consecutive days, 6 sessions on alternate days and then 3 weekly sessions until recovery of renal function and/or a reduction in FLC <500mg/L and/or after 6 weeks had elapsed, at which time an assessment was made of whether or not to continue treatment according to the patient's clinical evolution and response to chemotherapy.
Data analysis was performed using SPSS 15.0.
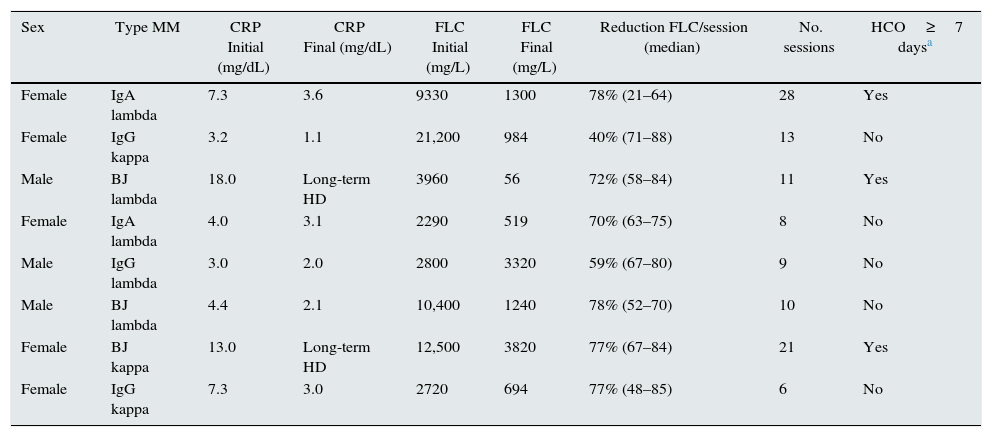
Eight patients were analysed (Table 1). Three were male (37%) and five female (62%), with mean age 67±9 years. Six patients (75%) had de novo multiple myeloma and two (25%) had relapses. One patient (12%) had a history of chronic kidney disease as a result of nephroangiosclerosis (eGFR by CDK-EPI: 49mL/min/1.73m2). The FLC were lambda in five patients (62%). Seven patients (87%) had renal involvement at the time of diagnosis and all required HD at the start of treatment. The median number of FLC at baseline was 3415mg/L (2740–11,975). In 3 patients (37%), HD with HCO was delayed ≥7 days from the time of diagnosis of acute renal failure.
Clinical data of patients treated with HD with HCO.
| Sex | Type MM | CRP Initial (mg/dL) | CRP Final (mg/dL) | FLC Initial (mg/L) | FLC Final (mg/L) | Reduction FLC/session (median) | No. sessions | HCO≥7 daysa |
|---|---|---|---|---|---|---|---|---|
| Female | IgA lambda | 7.3 | 3.6 | 9330 | 1300 | 78% (21–64) | 28 | Yes |
| Female | IgG kappa | 3.2 | 1.1 | 21,200 | 984 | 40% (71–88) | 13 | No |
| Male | BJ lambda | 18.0 | Long-term HD | 3960 | 56 | 72% (58–84) | 11 | Yes |
| Female | IgA lambda | 4.0 | 3.1 | 2290 | 519 | 70% (63–75) | 8 | No |
| Male | IgG lambda | 3.0 | 2.0 | 2800 | 3320 | 59% (67–80) | 9 | No |
| Male | BJ lambda | 4.4 | 2.1 | 10,400 | 1240 | 78% (52–70) | 10 | No |
| Female | BJ kappa | 13.0 | Long-term HD | 12,500 | 3820 | 77% (67–84) | 21 | Yes |
| Female | IgG kappa | 7.3 | 3.0 | 2720 | 694 | 77% (48–85) | 6 | No |
FLC: free light chains; ARF: acute renal failure; HCO: high-cut-off dialysers; HD: haemodialysis; MM: multiple myeloma.
Extended haemodialysis with Gambro HCO 2100 dialyser (Theralite®) was used in all cases.
A median of 10 extended HD sessions with HCO were performed per patient (8–19), with a mean reduction in FLC per session of 73% (61–77). In the last HD with HCO session, we observed a mean concentration of FLC (pre-dialysis) of 972mg/L (562–2815).
Six patients (75%) had an improvement in renal function, no longer requiring HD at the end of treatment. Two patients had no improvement in renal function and had to start long-term HD programmes. The start of treatment with HD with HCO had been delayed for more than seven days in both of these patients, one of whom was refractory to chemotherapy.
Among the patients who recovered renal function, we observed a median of 9 months free of HD (5–15). The mean follow-up time for each patient was 9 months (4–15). One patient died 11months after starting HD with HCO because the development of sepsis with multiple organ failure, having maintained stable renal function up to that time.
Mean albumin levels were 2.6±0.4g/dL, potassium 3.3±0.4mEquiv./L, phosphorus 2.9±0.6mg/dL, calcium 8.8±0.2mg/dL and magnesium 1.9±0.3mg/dL.
Patients tolerated the sessions satisfactorily from a haemodynamic point of view, and there were no incidents of note during the sessions.
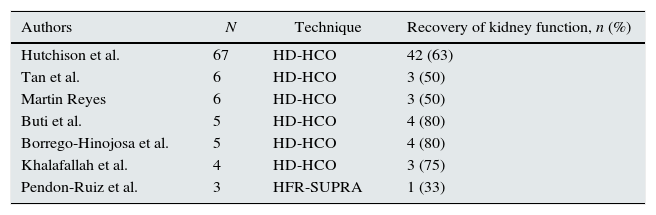
An increasing number of authors are proposing HD with HCO as effective adjuvant therapies in the treatment of myeloma kidney1–8 (Table 2). The advantage of these techniques is their high cut-off point, up to 60kD, which obtains greater clearance of the FLC.
Experience of different authors with haemodialysis in ARF and myeloma.
| Authors | N | Technique | Recovery of kidney function, n (%) |
|---|---|---|---|
| Hutchison et al. | 67 | HD-HCO | 42 (63) |
| Tan et al. | 6 | HD-HCO | 3 (50) |
| Martin Reyes | 6 | HD-HCO | 3 (50) |
| Buti et al. | 5 | HD-HCO | 4 (80) |
| Borrego-Hinojosa et al. | 5 | HD-HCO | 4 (80) |
| Khalafallah et al. | 4 | HD-HCO | 3 (75) |
| Pendon-Ruiz et al. | 3 | HFR-SUPRA | 1 (33) |
ARF: acute renal failure; HD-HCO: extended haemodialysis with high-cut-off dialysers; HFR-SUPRA: haemodiafiltration with ultrafiltrate regeneration by adsorption in resin.
The main limitation of these techniques is the lack of controlled, randomised studies. There are currently two European multicentre studies underway, EuLITE9 and MYRE,10 the results of which will provide more evidence on the use of these techniques.
Please cite this article as: Sáez MI, Camarero V, Rosales A, Hijazi B, Izquierdo MJ, Labrador J, et al. Fracaso renal agudo en pacientes con mieloma: Nuestra experiencia con hemodiálisis extendidas con dializadores de alto poro. Nefrología. 2017;37:429–431.



