
Diabetic kidney disease is the most common cause of advanced chronic kidney disease.1,2 However, the therapeutic options continue to be limited for patients with diabetic kidney disease on maintenance haemodialysis. GLP-1 receptor agonists (GLP-1 RA) contribute to improving blood glucose control by reducing glycated haemoglobin (HbA1c).3 Other beneficial effects include feeling full, weight loss, increased natriuresis, lower blood pressure, decreased albuminuria and slowing down the progression of diabetic kidney disease.4,5 Despite this, its use in haemodialysis is rare.
We present the case of a 56-year-old man with high blood pressure, chronic obstructive pulmonary disease, advanced chronic kidney disease on pre-dialysis, type 2 diabetes mellitus treated with 32 IU of insulin detemir, 3mg repaglinide and 5mg linagliptin a day, with HbA1c at 8.5% and BMI 36.5kg/m2. In January 2021, he started incremental haemodialysis with one session/week (240min) with an asymmetric cellulose triacetate dialyser (1.9 m2) (ATA®) due to uraemic symptoms, poor blood pressure control and moderate-severe hyperkalaemia. His serum creatinine was 6.97mg/dl (estimated glomerular filtration rate using the CKD-EPI formula, 8.48ml/min/1.73 m2), creatinine clearance (CrCl) and urea clearance (KrU) measured by 24-h urine 16 and 5.84ml/min/1.73 m2, respectively. His glomerular filtration rate measured by the half-sum of CrCl and KrU was 10.92ml/min/1.73 m2 and the albumin/creatinine ratio was 3200mg/g.
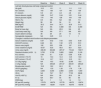
In order to optimise the patient's blood-glucose control, semaglutide (0.25mg/week) was added to the treatment, and linagliptin and repaglinide were discontinued. The doses were gradually increased to 1mg over 12 weeks, with good tolerance and no episodes of hypoglycaemia, and the insulin dose was gradually reduced. At 24 weeks, the patient's HbA1c had decreased by 23.5%, weight by 10.2% and BMI by 10.5%. In addition, not only did his fat mass and total body water decrease by 16.4% and 12.2% respectively, his lean mass increased by 14% (Table 1). His glomerular filtration rate remained unchanged throughout the observed period. However, the two parameters evolved differently, with KrU increasing and CrCl decreasing. Urinary creatinine excretion normalised to kilograms of weight increased, and urea remained stable. His blood pressure and albumin/creatinine ratio also decreased (Table 1).
Changes over time in lab test and haemodialysis parameters.
| Baseline | Week 4 | Week 8 | Week 12 | Week 24 | |
|---|---|---|---|---|---|
| Lab test, blood-glucose and body component control | |||||
| Hb (g/dl) | 10.5 | 10.1 | 11 | 11.1 | 11.2 |
| Na+ (mmol/l) | 143 | 136 | 137 | 140 | 139 |
| K+ (mmol/l) | 5.9 | 4.9 | 4.8 | 4.6 | 4.6 |
| Serum albumin (mg/dl) | 3.89 | 3.47 | 3.54 | 3.51 | 3.44 |
| Serum glucose (mg/dl) | 170 | 140 | 128 | 104 | 109 |
| HbA1c (%) | 8.5 | NA | NA | NA | 7.5 |
| Weight (kg) | 98 | 96 | 94 | 91 | 88 |
| BMI (kg/m2) | 35.2 | 34.4 | 33.7 | 32.6 | 31.5 |
| ECW/TBW | NA | NA | 0.389 | NA | 0.390 |
| Body fat mass (kg) | NA | NA | 29.9 | NA | 25 |
| Lean body mass (kg) | NA | NA | 57.1 | NA | 65.1 |
| Insulin detemir (IU/day) | 36 | 26 | 20 | 14 | 10 |
| Semaglutide (mg/week) | NA | 0.25 | 0.5 | 1 | 1 |
| Changes in residual renal function and dialysis parameters | |||||
| Serum creatinine (mg/dl) | 6.97 | 6.52 | 7.64 | 8.03 | 9.49 |
| CKD-EPI (ml/min) | 8.48 | 8.6 | 7.22 | 6.75 | 5.51 |
| Serum urea (mg/dl) | 192 | 203 | 208 | 197 | 219 |
| Urine creatinine (mg/dl) | 43.67 | 42.8 | 46.8 | 58.1 | 52.8 |
| Urine urea (mg/dl) | 436.39 | 664.86 | 497.37 | 719.44 | 738.71 |
| Residual diuresis (ml/24h) | 3,700 | 3,700 | 3,800 | 3,600 | 3,100 |
| KrU (ml/min) | 5.84 | 6.1 | 6.29 | 6.58 | 6.38 |
| CrCl (ml/min/1.73 m2) | 16 | 15.3 | 14.3 | 14.5 | 13.8 |
| GFR (ml/min/1.73 m2) | 10.9 | 10.7 | 10.3 | 10.5 | 10.1 |
| Cr U/kg (mg/kg) | NA | 16.5 | 18.92 | 22.98 | 18.6 |
| U U/kg (mg/kg) | NA | 256.25 | 201.07 | 284.61 | 260.23 |
| Bicarbonate (mmol/l) | 18.8 | 18.2 | 24.3 | 20 | 23 |
| nPCR (g/kg/day) | NA | 1.53 | 1.28 | 1.76 | 1.36 |
| ACR (mg/g) | 3,200 | 3,300 | 2,800 | 2,300 | 1,800 |
| VB (l) | NA | 76.7 | 78.7 | 77.33 | 96.86 |
| Vinf-OL-HDF (l) | NA | 26.4 | 26 | 25.3 | 29 |
| KT (l) | NA | 56.7 | 54 | 56 | 65 |
| IDWG (kg) | NA | 1 | 1.8 | 1.4 | 1.6 |
| BP pre-HD (mmHg) | 170/79 | 165/79 | 157/78 | 145/75 | 139/74 |
| BP post-HD (mmHg) | 193/87 | 182/81 | 172/79 | 163/78 | 155/78 |
ACR: albumin/creatinine ratio; BMI: Body Mass Index; BP: blood pressure; CrCl: 24h urine creatinine clearance; Cr U/kg: urinary creatinine excretion per kilo of weight; ECW/TBW: extracellular water/total body water ratio; GFR: glomerular filtration rate; Hb: haemoglobin; Hb1Ac: glycated haemoglobin; HD: haemodialysis; IDWG: interdialytic weight gain; K+: plasma potassium; KrU: renal clearance of residual urea; KT: efficacy of dialysis treatment; NA: not assigned; Na+: plasma sodium; nPCR: normalised protein catabolic rate; U U/kg: urinary urea excretion per kilo of weight; VB: volume of blood dialysed; Vinf-OL-HDF: infusion volume in online haemodiafiltration.
There are currently few case reports describing the use of semaglutide in patients on conventional haemodialysis6 and, to our knowledge, there are none on incremental haemodialysis regimens. This case describes for the first time the efficacy and safety of subcutaneous semaglutide in a patient with diabetes and obesity on incremental haemodialysis with a weekly session. We describe the favourable effects on blood-glucose control, the decrease in HbA1c, blood pressure control and the preservation of residual kidney function. Despite the satiating effect of the drug, protein intake is not reduced, as shown by the normalised protein catabolic rate (nPCR) of >1g/kg a day.
The latest Kidney Disease: Improving Global Outcomes (KDIGO) consortium clinical practice guidelines from 2020 on the management of diabetic kidney disease7 recommend prescribing GLP-1 RA due to their proven kidney and cardiovascular benefits, regardless of HbA1c levels. Semaglutide stimulates insulin and inhibits glucagon secretion from pancreatic islets in a glucose-dependent manner, leading to lower serum glucose levels. This agent can therefore be expected to have the same hypoglycaemic effect in haemodialysis patients and in the general diabetic population.
In our centre, the haemodialysis regimen is adjusted according to residual kidney function, and we consider an incremental regimen with a weekly session in patients with KrU>4ml/min/1.73 m2, as well as other criteria from the DIPPI study.8 In the patient described here, KrU was maintained, and even improved, during the follow-up period. His glomerular filtration rate did not increase as a result of the "apparent" decrease in CrCl, but this was due to the increase in lean mass, which leads to an increase in serum creatinine and a decrease in its clearance. In contrast, we found an interesting increase in both urea elimination and, in particular, the excretion of creatinine per kilogram of weight. This increased excretion could be partly due to an increase in tubular secretion, which would facilitate the elimination of other substances that are at present only eliminated by tubular secretion, such as protein-bound uraemic toxins. In addition, treatment with GLP-1 RA potentiates natriuresis, thereby improving blood pressure control. This, together with the weight loss, would explain the decrease in the albumin/creatinine ratio, which is crucial in maintaining residual kidney function.
Based on our experience, we believe that the use of GLP-1-RA in patients with diabetes and obesity helps achieve blood-glucose, weight and blood pressure control goals as well as providing other benefits on residual kidney function such as those described above. All of this would improve long-term morbidity and mortality in these patients and could facilitate their inclusion on kidney transplant waiting lists.
Ethical responsibilitiesThe study complied with the principles set out in the Declaration of Helsinki. The authors declare that they received the informed consent of the subject studied, and respect the patient's right to privacy. No experiments were performed on humans or animals for this study.
Conflicts of interestThe author has no conflicts of interest or financial support to declare.



