






The prevalence of cognitive impairment (CI) is high in hemodialysis patients. In this study, the relationship between CI and serum carnitine, plasma omega-3, omega-6 and omega-3/omega-6 fatty acid ratio was evaluated in hemodialysis patients.
Materials and methodsSixty two patients [male: 40 (64.5%), mean age 51±13 years] were included in this cross-sectional study. Serum total and free-carnitine levels were determined by ELISA. Plasma omega-3 [eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA)] and omega-6 [arachidonic acid (AA), dihomo gamma linoleic acid (DGLA)] levels were measured using LC-ESI-MS/MS. According to the Montreal Cognitive Assessment (MoCA) scores, ≤24 points were considered as CI. MoCA score ≤24 and >24 were determined as Group 1 and Group 2, respectively.
ResultsGroup 1 had significantly higher AA+DGLA/EPA+DHA ratios and lower free-carnitine, DHA and EPA+DHA levels compared to Group 2 (P=0.008, P=0.040, P=0.032, P=0.032, respectively). Group 1 had a statistically lower education level (P<0.05). Negative correlation was found between MoCA scores and AA+DGLA/EPA+DHA ratios (rs=−0.284, P=0.026). Free-carnitine levels were positively correlated with EPA and EPA+DHA levels (rs=0.278, P=0.030 and rs=0.271, P=0.034, respectively), and negative correlated with AA+DGLA/EPA+DHA ratios (rs=−0.414, P=0.001). In multivariate logistic regression analysis, MoCA scores was associated with AA+DGLA/EPA+DHA ratio (P=0.009) and education level (P<0.001).
ConclusionIt was determined that high AA+DGLA/EPA+DHA ratio and low education level could be independent risk factors of the CI. It has been shown that free-carnitine level can have positive effects on plasma EPA+DHA and AA+DGLA distributions. Low omega-3 fatty acid levels may be associated with CI in hemodialysis patients, and low carnitine level may contribute partially to this process. In addition, cognitive education programs may have an effect on preventing CI in hemodialysis patients with low education levels.
La prevalencia de deterioro cognitivo (CI) es alta en pacientes en hemodiálisis. En este estudio se evaluó la relación entre el CI y las proporciones de carnitina sérica, ácidos grasos omega-3, omega-6 y omega-3/omega-6 en plasma en pacientes en hemodiálisis.
Materiales y métodosEn este estudio transversal se incluyeron 62 pacientes (hombres: 40 [64,5%], edad media 51±13años). Los niveles séricos de carnitina total y libre se determinaron mediante ELISA. Los niveles plasmáticos de omega-3 (ácido eicosapentaenoico [EPA], ácido docosahexaenoico [DHA]) y omega-6 (ácido araquidónico [AA], ácido dihomo gamma linoleico [DGLA]) se midieron utilizando LC-ESI-MS/MS. Según las puntuaciones de la Evaluación Cognitiva de Montreal (MoCA), ≤24 indican CI. Las puntuaciones MoCA ≤24 y >24 se determinaron como grupo 1 y grupo 2, respectivamente.
ResultadosEl grupo 1 tenía proporciones de AA + DGLA/EPA + DHA significativamente más altas y niveles más bajos de carnitina libre, DHA y EPA +DHA en comparación con el grupo2 (p=0,008, p=0,040, p=0,032 y p=0,032, respectivamente). El grupo1 tenía un nivel educativo estadísticamente más bajo (p<0,05). Se descubrió una correlación negativa entre las puntuaciones de MoCA y las proporciones AA + DGLA/EPA + DHA (rs=−0,284, p=0,026). Los niveles de carnitina libre se correlacionaron positivamente con los niveles de EPA y EPA + DHA (rs=0,278, p=0,030, y rs=0,271, p=0,034, respectivamente), y negativamente con las proporciones AA +DGLA/EPA +DHA (rs=−0,414, p=0,001). En el análisis de regresión logística multivariante las puntuaciones de MoCA se asociaron con las proporciones AA +DGLA/EPA + DHA (p=0,009) y con el nivel educativo (p<0,001).
ConclusiónSe determinó que una alta relación AA +DGLA/EPA +DHA y un bajo nivel educativo podrían ser factores de riesgo independientes del CI. Se ha demostrado que el nivel de carnitina libre puede tener efectos positivos en las distribuciones plasmáticas de EPA + DHA y AA + DGLA. Los niveles bajos de ácidos grasos omega-3 pueden estar asociados con el CI en pacientes en hemodiálisis, y los niveles bajos de carnitina pueden contribuir parcialmente a este proceso. Además, los programas de educación cognitiva pueden tener un efecto en la prevención del CI en pacientes en hemodiálisis con bajos niveles educativos.
Cognitive impairment (CI) is chronic and progressive disablement of cognitive functions beyond what is expected in the normal aging process. CI may progress to dementia, and is associated with an increased risk of disability and health care expenditures.1 Chronic kidney disease (CKD) is an increased risk factor for CI and it has been demonstrated that there is a correlation between the severity of CKD and CI.2 Because, CI was detected in about 70% of middle-aged and elderly hemodialysis patients compared to the age-compatible general population.3 The probable causes of CI in this patient population are explained as vascular damage to brain tissue and direct neurotoxic effects of uremic toxins.4 Nowadays, the Montreal Cognitive Assessment (MoCA) can be used as a reliable method in the diagnosis and follow-up of CI in hemodialysis patients.5
l-Carnitine (3-hydroxy-4-N-trimethyl-aminobutyric acid), a low-molecular-weight amino acid derivative, is crucial for the-oxidation of long-chain fatty acids. It is the cofactor that mediates the entry of long-chain fatty acids into the mitochondria during the energy production process, and inhibits the accumulation of toxic fatty acids in the mitochondria in some pathological situations that can cause oxidative stres.6 Kidneys also play an important role in l-carnitine metabolism (expression, secretion, reabsorption).7 Carnitine hemostasis is disrupted in patients undergoing maintenance hemodialysis, and the carnitine level in plasma and tissues decreases due to both decreased protein intake and the removal of carnitine by dialysis.8
Omega-3 long chain polyunsature fatty acids are essential fatty acids, and their main source is sea foods. These fatty acids mediate a number of key biological processes such as eicosanoid production, the effects of cell membranes on signal transduction pathways, and modulation of inflammation. Long-chain omega-6 fatty acids are also essential fatty acids, are most abundant in meat and meat products, and have pro-inflammatory and pro-oxidant effects competitively against the anti-inflammatory effects of omega-3 fatty acids.9–11 It is emphasized that omega-3/omega-6 fatty acids balance is deteriorated in favor of omega-6 fatty acids due to decreases in some enzyme activities such as desaturase in hemodialysis patients,11 and this situation can be partially corrected by both omega-3 fatty acids12 and l-carnitine treatment.13 In previous studies on dialysis patients, calculations were made on the ratios of omega-3 and omega-6 fatty acids, especially due to their opposite effects on the inflammatory process.12–14 In addition, low plasma omega 3/omega-6 fatty acid ratios have been shown to be associated with CI.15
Recently, positive effects of l-carnitine16,17 and omega-3 fatty acids18,19 on cognitive functions have been reported. However, there is not enough data in the literature on the effect of carnitine and fatty acids on cognitive functions in patients with CKD. According to an experimental CKD rat model, it has been shown that administration of l-carnitine can provide a significant improvement in cognitive function.20 In a recent study in hemodialysis patients, it was emphasized that long-term l-carnitine treatment can reduce white matter microstructural damage and CI.21 We considered that carnitine and omega-3 fatty acids may have positive effects on CI observed in hemodialysis patients. Therefore, in the study, it was aimed to evaluate the relationship between serum total carnitine, free carnitine, and plasma omega-3 [eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)] and omega-6 [arachidonic acid (AA) and dihomo-gamma-linolenic acid (DGLA)] fatty acid levels and ratios with cognitive functions that was determined according to the MoCA in patients undergoing maintenance hemodialysis.
Material and methodStudy design and participantsSixty two patients undergoing maintenance hemodialysis in the nephrology clinic between March 2017 and February 2018 were included in this cross-sectional study. The study was designed in accordance with the 2018 Declaration of Helsinki, and was approved by the local ethics committee (Protocol date/number; 10.02.2017/2017-02). After all participants were informed about the study in detail, their written informed consent was obtained.
Communication insufficiency or visual, auditory and motor dysfunctions preventing MoCA test, cerebrovascular event, history of psychiatric (anxiety, depression, etc.) disease, frequent intradialytic hypotension attacks (systolic and/or diastolic blood pressures<90/50mmHg) non-compliance with HD treatment, severe anemia, decompensated heart failure, liver failure, active infection, thyroid dysfunction, malignancy, use of alcohol-narcotic drug, fish oil containing and antioxidant products were accepted as the exclusion criteria of this study.
Medical histories and demographic data were obtained from the medical records of the patients. Current medical treatments, smoking, co-morbid diseases, presence of renal residue, dialysis durations, systolic and diastolic blood pressures were recorded.
Hemodialysis protocols of the patients were applied as three times a week for 4h, dialysate flow rate 500mL/min and blood flow rate 250–350mL/min using bicarbonate dialysis solution and low/mid-flux polysulphone dialyzer (≥1.4ms). Body massindex (BMI) was calculated. The education levels of the patients were grouped as the first five years (primary school), 6–11 years (secondary school), and 12 and above (high school and university education), respectively. In addition, patients who received l-carnitine treatment (patients given 1g intravenous l-carnitine after each hemodialysis session for more than 3 months) due to muscle cramps that developed on dialysis, CKD-related anemia resistant to erythropoietin treatment, and weakness and those who did not receive l-carnitine treatment were determined.
Biochemical analysis proceduresBlood samples of the participants were taken after an overnight fasting, before the second hemodialysis session. After the MoCA test was performed, blood samples were taken as soon as possible. Blood samples taken into tubes with clota activator were kept at room temperature for 30min, and then centrifuged at 1310×g for 10min. Biochemical parameters were analyzed from the obtained serum samples [blood urea nitrogen, serum creatinine, glucose, sodium, potassium, calcium, phosphorus, bicarbonate, uric acid, albumin, alanine aminotransferase, lipids, ferritin, parathormone and c-reactive protein (CRP)]. While complete blood count analysis was performed with one of the blood samples taken into tubes containing K2-EDTA, the other K2-EDTA containing blood sample was used to get plasma sample after the centrifugation at 582×g for 10min. In addition, blood samples were taken into the tubes with clot activator at the end of dialysis to measure the post-dialysis blood urea nitrogen levels. Serum and plasma samples that were allocated for the determination of total/free carnitine, omega-3 and omega-6 fatty acid levels were stored at −80°C until the analysis day.
Beckman Coulter AU 5800 and MindrayBC-6800 devices were used for the measurement of routine biochemical and hematological parameters, respectively. Serum CRP level was measured by nephelometric method. Hemodialysis adequacy was determined by calculating single pool Kt/Vurea (spKt/Vurea) and urea reduction rates (URR).22
Human total and free carnitine serum concentrations were determined by the Enzyme-Linked Immunosorbent Assay (ELISA) method using commercially available kits (Shanghai YL Biotech Co., Ltd., Catalog No: YLA0451HU and Shanghai YL Biotech Co., Ltd., Catalog No: YLA0226HU). The intra-assay and inter-assay coefficients of variation for total and free serum carnitine assays were 8% and 10%, respectively. The sensitivity of total and free serum carnitine analyzes were 0.52nmol/mL and 0.21nmol/mL, respectively. Total and free serum carnitine test ranges were 1–300nmol/mL, and 0.5–200nmol/mL, respectively. Omega 3 and omega 6 fatty acids were measured using electrospray ionization (ESI) technique in multiple reaction monitoring (MRM) mode by the LC-MS/MS device (Thermo Scientific TSQ Quantum Access Max) by modifying the method of Valianpour et al.23
MoCA procedure and evaluationThe MoCA is a short screening test consisting of 12 items, lasting approximately 10–15min and achieving a maximum of 30 points, in which parameters such as visualspatial and executive functions (5 points), naming (3 points), language (3 points), attention (6 points), abstract thinking (2 points), short-term memory/recall (5 points), orientation (6 points) can be evaluated. The Turkish version of this test, which has been shown to be reliable and effective, was used in the study.24 Since the cognitive performance of hemodialysis patients may be affected by the fluid variability that occurs during dialysis, the MoCA tests were performed in a separate room before dialysis. While determining the MoCA score, similar to previous studies in hemodialysis patients, one point was added to the total score of those with an education level of ≤11 years, and ≤24 points were considered as CI.5,21 According to the total score of the MoCA, two groups were formed as ≤24 and >24, and then their demographic, clinical and laboratory characteristics were compared.
Statistical analysisIBM SPSS 23 package program was used for statistical analysis. Shapiro–Wilk test was used to determine whether the groups were normally distributed. While categorical variables were given as numbers and percentages, continuous variables with normal distribution were given as mean±standard deviation and continuous variables not showing normal distribution were given as median (25–75th quartile). While Student's t-test was used to determine whether the normally distributed continuous variables showed a statistically significant difference between the two groups, the Mann–Whitney U test was used to determine whether the continuous variables that did not show a normal distribution showed a statistically significant difference between the two groups. Spearman correlation analysis was performed to determine the relationships between parameters. Univariate and multivariate logistic regression analyses were used to determine which parameters affect the cognitive functions. P<0.05 was considered statistically significant.
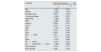
ResultsThe mean age of 62 hemodialysis patients (40 males, 64.5%) was 51±13 years. The number of patients with an education level of 12 years was 9 (14.5%), and the number of patients who received 1g of intravenous l-carnitine treatment after each hemodialysis session was 22 (35.5%). There was no statistically significant difference between total and free carnitine levels of patients who received l-carnitine treatment and those who did not [38.6 (14.4–93.4) nmol/mL vs. 33.1 (17.2–68.0) nmol/mL, P=0.971, and 26.4 (13.1–42.1) nmol/mL vs. 23.1 (15.3–40.1) nmol/mL, P=0.930, respectively]. The mean MoCA total score of all patients was 20.5. Details of the demographic, clinical and laboratory data of the patients are presented in Tables 1 and 2.
Basic characteristics of the patients.
| Variables | Patients (n=62) |
|---|---|
| Gender; male, n (%) | 40 (64.5) |
| Age, years | 51±13 |
| Residential (urban/rural), n (%) | 42/20 (67.7/32.3) |
| Education level, n (%) | |
| 1–5 years | 36 (58.1) |
| 6–11 years | 17 (27.4) |
| ≥12 years | 9 (14.5) |
| Hypertension, n (%) | 45 (72.6) |
| Diabetes Mellitus, n (%) | 14 (22.6) |
| Current smoker, n (%) | 22 (35.5) |
| Systolic blood pressure, mmHg | 129±24 |
| Diastolic blood pressure, mmHg | 78±13 |
| Body mass index, kg/m2 | 25.5±5.2 |
| Dialysis vintage, month | 52.5 (21.0–116.2) |
| Renal residual volume, n (%) | 17 (27.4) |
| Medical treatments, n (%) | |
| l-Carnitine | 22 (35.5) |
| Iron sucrose | 39 (62.9) |
| Erythropoietin | 43 (69.4) |
| Vitamin D | 18 (29) |
| Antiagregant | 30 (48.4) |
| Statin | 5 (8.1) |
| Phosphorus binder | 46 (74.2) |
| Montreal cognitive assessment (MoCA) score (point) | |
| Visual spatial/Executive (0–5) | 3 (2–5) |
| Naming (0–3) | 3 (2–3) |
| Attention (0–6) | 4 (2–4) |
| Language (0–3) | 1 (0–3) |
| Abstraction (0–2) | 1 (0–2) |
| Delayed recall (0–5) | 1 (0–2.3) |
| Orientation (0–6) | 6 (5–6) |
| Total score (0–30) | 20.5 (14.0–24.25) |
Categorical data are presented as frequencies and percentages; continuous variables are presented as mean±standard deviations or median and (25–75th quartile) depending on their distributions.
Laboratory characteristics of the patients.
| Variables | Patients (n=62) |
|---|---|
| BUN, mg/dL | 75±13 |
| Creatinine, mg/dL | 10.2 (7.9–11.6) |
| spKt/Vurea | 1.56±0.29 |
| URR, (%) | 72±6 |
| Glucose, mg/dL | 90 (81–125) |
| Sodium, mEq/L | 139±3 |
| Potassium, mEq/L | 5.4±0.6 |
| Calcium, mg/dL | 8.7±0.7 |
| Phosphorus, mg/dL | 5.4±1.3 |
| Albumin, g/dL | 3.9±0.3 |
| ALT, U/L | 10 (7–15) |
| Uric acid, mg/dL | 7.3±1.1 |
| Triglyceride, mg/dL | 174 (118–239) |
| LDL-C, mg/dL | 90 (73–115) |
| Bicarbonate, mmol/L | 21.3±2.6 |
| Hemoglobin, g/dL | 10.9±1.9 |
| Ferritin, ng/mL | 738 (507–1038) |
| Parathormone, pg/mL | 429 (253–696) |
| CRP, mg/dL | 6.0 (3.12–11.9) |
| Total carnitine, nmol/mL | 36.1 (16.4–79.3) |
| Free carnitine, nmol/mL | 25.0 (15.0–42.2) |
| EPA, mg/L | 15.3 (10.3–50.7) |
| DHA, mg/L | 28.2 (19.9–89.0) |
| EPA+DHA, mg/L | 54.8 (30.2–147.2) |
| DGLA, mg/L | 46.1 (29.2–80.2) |
| AA, mg/L | 137(90–377) |
| DGLA+AA, mg/L | 184 (114–644) |
| DGLA+AA/EPA+DHA | 4.51 (3.24–5.72) |
Categorical data are presented as frequencies and percentages; continuous variables are presented as mean±standard deviations or median and (25–75th quartile) depending on their distributions.
Abbreviations: AA, arachidonic acid; ALT, alanine aminotransferase; BUN, blood urea nitrogen; CRP, c-reactive protein; DGLA, dihomo-gamma lineloic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; LDL-C, low density lipoprotein cholesterol; spKt/V (üre), single pool Kt/Vure (urea kinetic model); URR, urea reduction rate.
In the MoCA test, when the threshold value for determining CI was taken as 24 points, the total score was found to be ≤24 in 43 (69.4%) of the patients (Group 1), while the total score was found to be >24 in 19 (30.6%) of the patients (Group 2). In Group 1, the female gender was statistically significantly higher (P=0.006), and education levels were significantly lower (1–5 years, P<0.001; 6–11 years, P=0.019; ≥12 years, P=0.002, respectively.). While there was no statistically significant difference for l-carnitine treatment between the groups (P=0.669), serum free carnitine levels were found to be statistically significantly higher in Group 2 (P=0.040). However, although the serum total carnitine level was numerically higher in Group 2, it did not reach statistical significance (P=0.072). While plasma DHA and EPA+DHA levels were statistically significantly higher in Group 2 (P=0.032, P=0.032, respectively), plasma AA+DGLA/EPA+DHA ratio was found to be statistically significantly lower (P=0.008). In addition, all specific cognitive function scores of Group 1 were statistically significantly lower than Group 2 (P<0.05). Details of demographic and clinical data between groups are shown in Tables 3 and 4.
Comparison of demographic and somatometric data of the groups.
| Variables | Group 1 (n=43) | Group 2 (n=19) | P |
|---|---|---|---|
| Gender; male, n (%) | 23 (53.5) | 17 (89.5) | 0.006 |
| Age, years | 51.5±12.3 | 46.1±13.2 | 0.144 |
| Residential (urban/rural), n (%) | 30/13 (69.8/30.2) | 12/7 (63.2/36.8) | 0.608 |
| Education level, n (%) | |||
| 1–5 years | 33 (76.7) | 3 (15.8) | <0.001 |
| 6–11 years | 8 (18.6) | 9 (47.4) | 0.019 |
| ≥12 years | 2 (4.7) | 7 (36.8) | 0.002 |
| Hypertension, n (%) | 32 (74.4) | 13 (68.4) | 0.626 |
| Diabetes Mellitus, n (%) | 9 (20.9) | 5 (26.3) | 0.744 |
| Current smoker, n (%) | 14 (32.6) | 8 (42.1) | 0.469 |
| Systolic blood pressure, mmHg | 130±27 | 124±18 | 0.341 |
| Diastolic blood pressure, mmHg | 78±14 | 77±10 | 0.818 |
| Body mass index, kg/m2 | 25.4±5.03 | 25.8±5.79 | 0.786 |
| Dialysis vintage, month | 60 (12–120) | 52 (25–96) | 0.593 |
| Renal residual volume, n (%) | 10 (23.3) | 7 (36.8) | 0.269 |
| Medical treatments, n (%) | |||
| l-Carnitine | 16 (37.2) | 6 (31.6) | 0.669 |
| Iron sucrose | 28 (65.1) | 11 (57.9) | 0.587 |
| Erythropoietin | 32 (74.4) | 11 (57.9) | 0.193 |
| Vitamin D | 12 (27.9) | 6 (31.6) | 0.769 |
| Antiagregan | 19 (44.2) | 11 (57.9) | 0.879 |
| Statins | 5 (11.6) | 0 (0) | 0.312 |
| Phosphorus binder | 30 (69.8) | 16 (84.2) | 0.347 |
| Specific cognitive functions (point) | |||
| Visualspatial/executive | 3 (1–3) | 5 (4–5) | <0.001 |
| Naming | 3 (2–3) | 3 (3–3) | 0.005 |
| Attention | 3 (1–6) | 6 (5–6) | <0.001 |
| Language | 1 (0–2) | 3 (2–3) | <0.001 |
| Abstraction | 0 (0–1) | 2 (2–2) | <0.001 |
| Delayed recall | 0 (0–2) | 2 (1–4) | <0.001 |
| Orientation | 6 (5–6) | 6 (6–6) | 0.002 |
Categorical data are presented as frequencies and percentages; continuous variables are presented as mean±standard deviations or median and (25th-75th quartile) depending on their distributions.
Comparison of the laboratory data of the groups.
| Variables | Group 1 (n=43) | Group 2 (n=19) | P |
|---|---|---|---|
| BUN, mg/dL | 75±12 | 74±13 | 0.700 |
| Creatinine, mg/dL | 9.3±2.4 | 10.8±2.3 | 0.031 |
| spKt/Vurea | 1.6±0.32 | 1.48±0.17 | 0.053 |
| URR, (%) | 72±7.1 | 71±4.6 | 0.347 |
| Glucose, mg/dL | 89 (79–122) | 106 (82–29) | 0.479 |
| Sodium, mEq/L | 139±3.5 | 140±2.0 | 0.223 |
| Potassium, mEq/L | 5.38±0.66 | 5.31±0.51 | 0.676 |
| Calcium, mg/dL | 8.64±0.74 | 8.78±0.61 | 0.479 |
| Phosphorus, mg/dL | 5.42±1.27 | 5.43±1.33 | 0.976 |
| Albumin, g/dL | 3.84±0.32 | 4.06±0.33 | 0.020 |
| ALT, U/L | 10 (7–15) | 10 (7–14.5) | 0.782 |
| Uric acid, mg/dL | 7.2±1.2 | 7.4±0.9 | 0.396 |
| Triglyceride, mg/dL | 167 (101–235) | 191 (125–333) | 0.255 |
| LDL-c, mg/dL | 82 (67–107) | 115 (80–132) | 0.014 |
| Bicarbonate, mmol/L | 21.5±2.74 | 20.7±2.19 | 0.215 |
| Hemoglobin, g/dL | 10.7±2.1 | 11.5±1.2 | 0.110 |
| Ferritin, ng/mL | 417 (250–640) | 471 (269–713) | 0.468 |
| Parathormone, pg/mL | 417 (250–640) | 471 (269–713) | 0.879 |
| CRP, mg/dL | 6.5 (3.1–16.3) | 4.7 (1.4–8.3) | 0.044 |
| Total carnitine, nmol/mL | 21.7 (13.1–39.4) | 37.1 (17.8–46.6) | 0.072 |
| Free carnitine, nmol/mL | 12.8 (10.3–34.0) | 36.6 (10.9–113) | 0.040 |
| EPA, mg/L | 12.8 (10.3–34.0) | 36.6 (10.9–113) | 0.094 |
| DHA, mg/L | 23.8 (18.3–67.9) | 67.4 (29.2–243) | 0.032 |
| EPA+DHA, mg/L | 39.2 (29.1–107) | 96.0 (48.8–243) | 0.032 |
| DGLA, mg/L | 49.8 (35.5–89.0) | 40.3 (17.1–64.6) | 0.075 |
| AA, mg/L | 136 (103–380) | 145 (69–269) | 0.275 |
| DGLA+AA, mg/L | 184 (140–473) | 185 (96–337) | 0.242 |
| AA+DGLA/EPA+DHA | 4.74 (3.62–5.88) | 3.37 (0.51–4.66) | 0.008 |
Categorical data are presented as frequencies and percentages; continuous variables are presented as mean±standard deviations or median and (25–75th quartile) depending on their distributions.
Abbreviations: AA, arachidonic acid; ALT, alanine aminotransferase; BUN, blood urea nitrogen; CRP, c-reactive protein; DGLA, dihomo-gamma lineloic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; LDL-C, low density lipoprotein cholesterol; spKt/V (üre), single pool Kt/Vure (urea kinetic model); URR, urea reduction rate.
When the comparison was made by gender, statistically significant lower MoCA score, education level, serum creatinine level (P<0.001, P=0.003, P=0.005, respectively), and higher spKt/Vurea and URR were detected in women (P<0.001, P<0.001, respectively). The plasma AA+DGLA/EPA+DHA ratio was found to be significantly higher in women [4.12 (2.63–5.69) vs. 4.76 (4.29–5.81), P=0.050].
When correlation analysis of variables associated with MoCA total scores was performed, age (rs=−0.410, P=0.001), gender (rs=−0.538, P<0.001), education level (rs=0.694, P<0.001)), spKt/Vure (rs=−0.398, P=0.001), URR (rs=−0.390, P=0.002), albumin (rs=0.296, P=0.019) and plasma AA+DGLA/EPA+DHA ratio (rs=−0.284, P=0.026) were found to be correlated. There was no statistically significant correlation between MoCA total scores and taking l-carnitine treatment, serum total and free carnitine levels. (rs=−0.083, P=0.521; rs=0.176, P=0.171; rs=0.206, P=0.108, respectively). However, there was a statistically significant positive correlation between serum free carnitine levels and plasma EPA and EPA+DHA levels (rs=0.278, P=0.030 and rs=0.271, P=0.034, respectively). In addition, statistically significant negative correlation was found between serum total and free carnitine levels and plasma AA+DGLA/EPA+DHA ratio (rs=−0.363, P=0.004 and rs=−0.414, P=0.001, respectively). Details of the correlation analyzes mentioned above are presented in Tables 5 and 6.
Correlation analysis of MoCA total scores and variables.
| Variables | MoCA total scores (n=62) | |
|---|---|---|
| rs | P | |
| Age | −0.410 | 0.001 |
| Gender | −0.538 | <0.001 |
| Education level | 0.694 | <0.001 |
| l-Carnitine therapy | −0.083 | 0.521 |
| spKt/Vurea | −0.398 | 0.001 |
| URR | −0.390 | 0.002 |
| Albumin | 0.296 | 0.019 |
| LDL-C | 0.214 | 0.101 |
| CRP | −0.190 | 0.140 |
| EPA | 0.109 | 0.402 |
| DHA | 0.225 | 0.081 |
| EPA+DHA | 0.211 | 0.102 |
| AA | −0.111 | 0.396 |
| DGLA | −0.214 | 0.098 |
| AA+DGLA | −0.131 | 0.316 |
| AA+DGLA/EPA+DHA | −0.284 | 0.026 |
| Total carnitine | 0.176 | 0.171 |
| Free carnitine | 0.206 | 0.108 |
Significance was determined by Sperman rank correlation coefficient.
Abbreviations: AA, arachidonic acid; CRP, c-reactive protein; DGLA, dihomo-gamma lineloic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; LDL-C, low density lipoprotein cholesterol; spKt/V (üre), single pool Kt/Vure (urea kinetic model); URR, urea reduction rate.
Correlation analysis of serum carnitine levels with fatty acids.
| Total carnitine | Free carnitine | |||
|---|---|---|---|---|
| Variables | rs | P | rs | P |
| EPA | 0.211 | 0.102 | 0.278 | 0.030 |
| DHA | 0.185 | 0.153 | 0.245 | 0.057 |
| EPA+DHA | 0.204 | 0.114 | 0.271 | 0.034 |
| AA | 0.021 | 0.872 | 0.054 | 0.679 |
| DGLA | 0.021 | 0.872 | 0.049 | 0.706 |
| AA+DGLA | 0.014 | 0.916 | 0.047 | 0.717 |
| AA+DGLA/EPA+DHA | −0.363 | 0.004 | −0.414 | 0.001 |
Significance was determined by Sperman rank correlation coefficient.
Abbreviations: AA, arachidonic acid; DGLA, dihomo-gamma lineloic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid.
When logistic regression analyses are performed, MoCA total score has a significant relationship with gender (P=0.013), education level (P<0.001), albumin (P=0.027), EPA (P=0.034), DHA (P=0.045), EPA+DHA (P=0.031) and AA+DGLA/EPA+DHA ratio (P=0.002) in univariate logistic regression analysis, whereas in multivariate logistic regression analysis MoCA total score was correlated with education level (P<0.001 and AA+DGLA/EPA+DHA ratio (P=0.009) (Table 7).
Variables associated with MoCA total score in univariate and multivariate logistic regression analysis.
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR (%95 CI min-max) | Wald | P | OR (%95 CI min-max) | Wald | P | |
| Gender | 7.391 (1.518–35.991) | 6.134 | 0.013 | |||
| Education level | 7.154 (2.645–19.351) | 15.020 | <0.001 | 6.292 (2.276–17.397) | 12.563 | <0.001 |
| Albumin | 8.967 (1.287–62.496) | 4.903 | 0.027 | |||
| EPA | 1.011 (1.001–1.021) | 4.479 | 0.034 | |||
| DHA | 1.010 (1.000–1.019) | 4.033 | 0.045 | |||
| EPA+DHA | 1.006 (1.001–1.011) | 4.645 | 0.031 | |||
| AA+DGLA/EPA+DHA | 0.575 (0.407–0.813) | 9.793 | 0.002 | 0.585 (0.390–0.877) | 6.739 | 0.009 |
Abbreviations: AA, arachidonic acid; DGLA, dihomo-gamma lineloic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; CI, confidence interval; OR, odds ratio (estimated).
In this study, it was determined that CI was common according to the MoCA test in patients undergoing maintenance hemodialysis. This result was similar to previous studies in which cognitive function assessment was performed with the same method in hemodialysis patients.5,25 It was shown that CI was correlated with age, gender, education level, dialysis efficiency, albumin level and AA+DGLA/EPA+DHA ratio. However, it was found that the relationship between education level and AA+DGLA/EPA+DHA ratio with cognitive impairment continued in the other variable adjustments were done.
In our study, similar to previous studies, it was shown that low education level is associated with poor cognitive function.5,25 The significant gender difference between the groups can be explained by the fact that the education level of women in the study is lower than that of men, and this situation negatively affects the cognitive functions of women. In general population based studies, it is emphasized that CI is higher in women compared to men,26 and this may be related to the socioeconomic status.27 Although our study results show that education level has an important effect on cognitive functions, it suggests that there are other risk factors for CI in this patient population, especially in women.
Another result of our study is that the spKt/Vurea and URR values were higher in Group 1 and women, although they did not reach statistical significance. In addition, negative correlations were found between MoCA total scores and spKt/Vurea and URR values in all patients. These results show that increased dialysis dose is not associated with better cognitive function, and even similar to the results of previous studies, high Kt/Vurea value may be associated with worse cognitive function.28,29 The authors stated that this finding can be explained by the fact that patients with high Kt/Vurea were generally weaker than normal and had worse nutrition. In our study, it was determined that low serum albumin level, which is an important indicator of poor nutritional status in hemodialysis patients,30 may be associated with CI. It was also considered that wide fluctuations in fluid, osmolarity and uremic toxin levels that may occur due to more intense hemodialysis in these patients may adversely affect cognitive functions. This relationship between serum albumin level, dialysis dose and cognitive functions was not observed in logistic regression analyses. However, the data support that higher spKt/Vurea is not associated with better cognitive function.
Carnitine, an essential cofactor for normal fatty acid metabolism, has shown beneficial effects on brain tissue. l-carnitine is known to contribute to the formation of acetyl carnitine and acetylcholine by mediating the passage of acetyl particles from mitochondria to cytosol in brain tissue.16 Acetyl carnitine shows neurobiological effects with synaptic morphology, synaptic transmission of many neurotransmitters, phospholipid metabolism, and brain energy modulation.31 It has been demonstrated that l-carnitine treatment can affect the central nervous system, and slow down CI by increasing serum concentrations of both l-carnitine and acetyl carnitine.32 It has been shown that serum carnitine levels of patients undergoing maintenance hemodialysis are significantly lower.8 In a study of Zhang et al.,33 it was emphasized that low total and free carnitine levels in hemodialysis patients can increase with l-carnitine treatment, and dialysis related complications can be reduced by determining the appropriate plasma free carnitine level. The data of our study suggest that low serum free carnitine level may be associated with poor cognitive functions. Also, the fact that carnitine levels were not different between those who received and did not receive l-carnitine therapy, suggesting that those who received l-carnitine therapy had lower carnitine levels at the beginning of treatment. In an experimental study on this subject, it was shown that administration of l-carnine to rats with CKD provided significant improvement in cognitive functions, and it was stated that this effect could be achieved by the antioxidant property, the energy need of the cells, and regulating the changes in membrane phospho lipid metabolism.20 In a recent study, it was revealed that l-carnitine may exert a neuroprotective effect by suppressing neuroinflammation against white matter microstructural damage and cognitive deterioration in hemodialysis patients.21 Although the available data support the use of l-carnitine in the treatment of CI in this patient population, the mechanisms of the effect of l-carnitine on cognitive functions should be revealed in detail.
Nowadays, it is stated that EPA and DHA can have neuroprotective effects. In brain tissue, DHA, main long-chain fatty acid of phospholipids, may prevent or correct CI when they are taken with diet for a long time.18,19 In hemodialysis patients, it was found that plasma omega-3/omega-6 fatty acid distribution changes abnormally, and plasma/cell phospholipids have lower EPA and DHA concentration.17,34 It was thought that this situation may be related to the scarcity of sea food taken in the diet of hemodialysis patients, the decrease in the functions of elongase and desaturase enzymes, malabsorption, and omega-3 fatty acid loss from dialysate.35,36
In our study, a significant relationship was found between lower MoCA scores and high AA+DGLA/EPA+DHA ratio in hemodialysis patients. This finding supports that there may be a relationship between the decrease in omega-3 fatty acid ratios and CI in hemodialysis patients. In addition, higher AA+DGLA/EPA+DHA ratio in females compared to males in our study may contribute causally to higher CI in females. Possible reasons for this situation are, as stated in a recent study, lower consumption of food containing omega-3 fatty acids in women,36 worse nutritional status of female patients lower serum albumin levels or greater omega-3 fatty acid loss with higher dialysis dose related dialysate. The positive correlation of serum free carnitine level with EPA and DHA, and negative correlation with AA+DGLA/EPA+DHA ratio show that l-carnitine can also be effective on the regulation of omega-3 fatty acid metabolism and the preservation of cognitive functions.
Our study has some limitations. It is difficult to generalize according to our findings, since it is a single-center, non-randomized study with a relatively small sample size. In addition, due to its cross-sectional design, cause and effect association should be done carefully. In our study, it was accepted that cognitive functions were impaired in patients with a MoCA total score of 24 points, and no distinction was made between mild-moderate CI and dementia, since patients with dementia were excluded from the study. Although there was no statistical difference in the proportions of patients receiving l-carnitine therapy between the groups, receiving this therapy likely affected serum total and free carnitine levels. Finally, since plasma fatty acid distribution may be affected by diet and dietary fatty acid intake, this could be further evaluated with nutritional intake analyzes. Despite these limitations, the specificity of the study group constitutes the strength of our study.
ConclusionAs a result, the prevalence of CI according to the MoCA was found to be high in hemodialysis patients. Low education level and high plasma AA+DGLA/EPA+DHA ratio were determined to be independent risk factors associated with CI. It has been shown that serum carnitine levels may have positive effects on plasma EPA+DHA and AA+DGLA distributions in these patients. According to our findings, it can be said that low omega-3 fatty acid levels in hemodialysis patients may be associated with the onset and progression of CI, and that low carnitine levels may partially contribute to this process. Assessment of cognitive functions in these patients especially those with low education level can be included in routine clinical practice, and symptoms associated with CI can be improved with omega-3 fatty acid and carnitine supplementation in patients with CI. In addition, data support that cognitive education programs should be applied to prevent or reduce cognitive impairment in hemodialysis patients with low education levels. However, our findings should be confirmed by prospective studies with large participation.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interestThe authors declare that they have no conflict of interests.



