




Post-dilution on-line hemodiafiltration (OL-HDF) is the most efficient infusion mode to obtain maximum clearances of uremic toxins, with a recommended manual infusion flow (Qi) of 25% of the blood flow with the main limitation that causes alarms by hemoconcentration throughout the session. Recent technical advances allow automatic prescription of Qi if hematocrit and total protein (TP) values are specified. As these analytical results are not possible to obtain in each dialysis session, a practical way to prescribe Qi is to make an automatic prescription adjusting the hematocrit and total protein values at the beginning of the session to obtain the manual prescription required and we will call it automatic-manual prescription. The aim of this study was to compare manual Qi with automatic- manual Qi in postdilution OL-HDF. 30 patients (16 men and 14 women), 59.9 ± 15 years old, in hemodialysis program for 50.1 ± 67 months were included. Every patient underwent four OL-HDF sessions, two with manual Qi (4008-S and 5008 monitors) and two with automatic- manual Qi (A-M), one with the same Qi and one with manual Qi +20 (A-M+20). The same usual dialysis parameters were maintained: helixone dialyzer, dialysis time of 266 ± 39 minutes, blood flow of 420 ± 36. Recirculation, Kt and intradialysis alarms were measured at each session. No significant differences in the fistula recirculation or dialysis dose measured using Kt. Total infusion volume was 24.9 ± 4 (4008S), 23.4 ± 4 L (5008) with manual Qi, 23.6 ± 4 L (A-M) Qi (NS) and 25.8 ± 5 L (A-M+20). Only 14% of patients had no incidents. The number of alarms was significantly higher with manual prescription 55 alarms with 4008 and 40 with 5008 vs. AM (11) p <0.01) and A-M+20 (16 alarms) We concluded that automatic-manual Qi is a practical way for post-dilutional OL-HDF prescription where the same efficiency and total reinfusion volume with an important reduction of intradialysis alarms are obtained, allowing to rise Qi by 20% without increasing intradialysis alarms.
La hemodiafiltración on-line (HDF-OL) posdilucional es la modalidad más eficaz para obtener la máxima depuración de toxinas urémicas, con un flujo de infusión (Qi) recomendable del 25% del flujo sanguíneo y con el principal inconveniente de provocar alarmas por hemoconcentración a lo largo de la sesión. Recientes avances técnicos permiten la prescripción automática del Qi si se especifican los valores del hematocrito y de las proteínas totales. Como no es posible disponer en cada sesión de estos valores, una forma práctica de pautar la HDF-OL posdilucional es realizar una prescripción automática ajustando el hematocrito y las proteínas totales para obtener al inicio de la sesión la prescripción manual prescrita, a la que llamaremos prescripción manual automatizada. El objetivo del estudio fue comparar la pauta convencional de Qi manual respecto a la manual automatizada. Se incluyeron 30 pacientes (16 varones y 14 mujeres), de 59,9 ± 15 años de edad, en programa de hemodiálisis durante 50,1 ± 67 meses. Cada paciente recibió cuatro sesiones de HDF-OL, dos con Qi manual (monitores 4008-S y 5008) y dos con Qi manual automatizada (M-A), una con Qi igual a la manual y otra incrementando el Qi 20 ml/min (M-A+20). El resto de parámetros de diálisis no variaron: filtro de helixona, tiempo de diálisis 266 ± 39 minutos, flujo de sangre 420 ± 36 ml/min. En cada sesión se recogieron el Kt, la recirculación y las alarmas. No se observaron diferencias significativas en el índice de recirculación ni en la dosis de diálisis medida con el Kt. El volumen total de infusión fue de 24,9 ± 4 l (4008S), 23,4 ± 4 l (5008) con Qi manual, 23,6 ± 4 l (M-A) y 25,8 ± 5 l (M-A+20). En sólo el 14% de los pacientes no hubo incidencias. El número de alarmas fue significativamente superior con la prescripción manual, 55 alarmas con 4008 y 40 con 5008, respecto a la M-A (11, p <0,01) y M-A+20 (16 alarmas). Concluimos que la prescripción del Qi manual automatizada es una forma práctica de prescribir la HDF-OL posdilucional consiguiendo el mismo volumen convectivo y la misma eficacia, con una importante reducción de las alarmas intradiálisis, lo que permite un incremento del Qi un 20% sin aumento del número de alarmas.
INTRODUCTION
Haemodiafiltration (HDF) with high levels of replacement fluid is an established renal replacement therapy that has undergone sustained growth over the last few years, since it achieves optimal elimination of uraemic toxins. Currently, postdilution on-line haemodiafiltration (OL-HDF) has been shown to be the most effective infusion mode to obtain the maximum clearance of uraemic toxins, with a recommended infusion flow (Qi) of 25% of the blood flow (Qb). The main limitation has been the number of alarms during sessions as a result of haemoconcentration.1-5
Recent technical advances and last generation monitors make it possible to automatically prescribe Qi if haematocrit values (Ht) and total protein (TP) are specified; Qi is automatically regulated throughout treatment. As it is not possible to know the values of Ht and TP for each session, a practical manner of determining postdilution OL-HDF is to prescribe automatically, by adjusting the values of Ht and TP at the beginning of each session, to obtain the indicated manual prescription, which we will name automated manual prescription (A-M). In this way, we have drawn up replacement therapy guidelines that have the advantage of using automatic auto-regulation.
The aim of this study was to compare postdilution OLHDF obtained using conventional manual Qi with that obtained using automated manual Qi.
MATERIALS AND METHODS
A prospective study was carried out on 30 patients (16 men and 14 women), of 59.9 ± 15 years of age, with a mean period in a haemodialysis program (HD) of 50.1 ± 67 months. The causes of chronic renal failure were: 8 vascular nephropathy, 3 chronic glomerulonephritis, 4 adult polycystic kidney, 2 tubulointerstitial nephritis, 3 diabetic nephritis, 3 systemic disease, 2 due to urological causes and 5 unknown. Each patient underwent 4 (midweek) sessions of postdilution OL-HDF, two with a manual Qi (one with a 4008-S monitor and the other with a 5008 monitor) and two with an automated manual Qi, both with 5008 monitors, one with a Qi equal to the manual one (M-A) and another with an increase in Qi of 20ml/min (M-A+20). To prescribe manual Qi, the replacement rate is adjusted to medical prescription (normally 25% of the Qb indicated) without pressing the automatic button. To prescribe M-A Qi, it is necessary, in the first place, to achieve the Qb indicated, then to activate the automatic button, subsequently TP and Ht values will be adapted to achieve the infusion flow indicated. In the case of M-A+20, the same procedure is followed as with M-A, but we will modify the values of TP and Ht until an initial infusion flow is obtained equal to the one indicated plus 20ml/min.
The order of each of the four sessions was random. The other dialysis parameters did not vary: 1.5 or 1.8m2 helixone filters, time of dialysis 266 ± 39 minutes, blood flow 420 ± 36ml/min, with a dialysate flow of 800ml/min. Dry weight was 65.3 ± 13kg, and the vascular access used was an A-V autologous fistula in 20 patients, a PTFE graft in 1 patient and tunnelised central catheters in 9 patients. In each session Kt was registered and the initial and final recirculation index. Furthermore, the blood pressure, venous pressure, transmembrane pressure (TMP) or haemoconcentration alarms were monitored.
The results are expressed as mean ± standard deviation. For the statistical significance analysis of the quantitative parameters, ANOVA has been used for paired data. A p < 0.05 was considered significant.
RESULTS
One-hundred and twenty sessions of OL-HDF were carried out, without any significant incidents, with the exception of a broken filter 5 minutes before the end of one session. Total protein and Ht mean values obtained during the last control analysis were 6.6 ± 0.6 g/dl and 35.9 ± 3.7%, respectively (although these data were not used to modify the monitor). No differences in initial weight were seen in the four sessions: 67.4 ± 14 (manual 4008), 67.6 ± 14 (manual 5008), 67.4 ± 13 (M-A) and 67.4 ± 13 (M-A+20), or in final weight: 65.0 ± 13, 65.3 ± 13, 65.1 ± 13 and 65.3 ± 13, respectively.
Nor were any differences detected in initial or final recirculation rate in the 3 sessions performed with monitor 5008, 12.5 ± 4% and 13.9 ± 5% (manual 5008), 11.9 ± 4% and 14.6 ± 6% with M-A, and 13.1 ± 5% and 13.3 ± 6% with M-A+20, respectively.
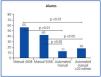
The mean value for Qi prescribed was 98.7 ± 10ml/min (with an interval of 80-110ml/min) in the manual sessions and M-A, and in the M-A+20 was 118.7 ± 10ml/min (with an interval of 100-130ml/min). The total infusion volume was 24.9 ± 4 (4008S) and 23.4 ± 4L (5008) with manual Qi (p < 0.01). Total infusion volume was 23.6 ± 4L with M-A and 25.8 ± 5L with M-A+20 (Figure 1).
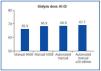
The dialysis dose determined by ionic dialysance was determined for total Kt obtained at the end of the session, and no significant differences were found (Figure 2). With reference to the presentation or not of alarms during dialysis, in Figure 3 it is possible to see the total number of alarms according to the modality of each session. Although 4 patients (14%) did not have any incidents of alarms, in the case of those patients that did, the number of alarms was significantly greater with manual prescription with 4008 (1.83 ± 2.6 alarms/session) or manual prescription with 5008 (1.33 ± 1.5 alarms/session) with respect to M-A (0.37 ± 0.7 alarms/session, p < 0.01) and even when M-A+20 was prescribed (0.53 ± 1.2 alarms/session, p < 0.01). There were no significant differences between the prescription of M-A and M-A+20ml/min. The alarms with the 4008 monitor were due to venous pressure 33 (60%) and TMP 22 (40%), whereas with the 5008 monitor the alarms were due to haemoconcentrations of more than 90% (Figure 4).
DISCUSSION
Given the latest technical advances available in last generation monitors and the progressive generalisation of HDF techniques, in this study we compare different options for Qi prescription in postdilution OL-HDF. In an analysis of 30 patients, each of which underwent two manual Qi sessions and two M-A Qi sessions (one with a Qi equal to manual and the other with an increased Qi of M-A+20), it was seen that with M-A Qi prescription the same convective volume and the same efficacy were obtained, with a significant reduction of alarms during dialysis, which made it possible to increase Qi without increasing the number of alarms.
Large multicentric observational studies, adjusted for demographic factors and comorbidities, have shown a reduction of mortality of 35% in patients who underwent HDF with more than 15 litres of replacement fluid.6-7 The prospective observational study RISCAVID8 has also shown, in patients that were undergoing OL-HDF, a reduction in mortality in comparison with those patients that underwent HDF with replacement bags, and this was even more significant in comparison with those that underwent HD. Furthermore, a comparative long term study,9 in 232 patients predominantly in an OL-HDF programme in comparison with 626 patients in a high-flux HD programme, showed a RR of death of 0.45. Several randomised, multicentric ongoing studies compare low to high-flux HD with OL-HDF with pre- or postdilution infusion.
With reference to the mode of infusion, postdilution OLHDF is currently the most used method, since there is high clearance of small and large solutes, even when this mode can cause a greater number of complications related to haemoconcentration and TMP.10 Although the postdilution mode partially solves technical problems, it also reduces the transference of solutes as a consequence of haemodilution.11,12 «Mid»-dilution is a recent alternative with infusion of half the dialyser, the first part as a postdilution HDF and the second half as a predilution HDF, showing similar results or even better ones than the postdilution mode.13,14 We are waiting for the practical application and results of mixed HDF, with simultaneous pre- and postdilution and autoregulation of both flows, which could optimise efficacy and prevent the disadvantages of haemoconcentration.15
In this way, HD research is currently directed to obtaining safer, more practical and effective systems, and this depends, to a large extent, on technical advances to improve the monitors. Concretely, to adjust the replacement rate of a manual postdilution OL-HDF treatment, the recommended Qi is 25% of Qb. Some of these monitors (Fresenius 5008) offer the possibility of automatically adjusting Qi after applying the following formula, in which it is necessary to use real values for TP and Ht.
Qi < Qb [1- Ht /100 ]. [1- (7·TP)/100 ]–TUF
TUF: Ultrafiltration rate (ml/min)
This result is adjusted by multiplying by a factor related to the dialyser, between 0.65-1.25, according to the internal diameter of the capillary fibres. Furthermore, during the first minutes of the dialysis session, the ultrafiltration coefficient is measured (Kuf), and subsequently, this is measured every hour or additional measurements are performed if there is any unexpected event; the cyclic pressure test is performed, which estimates and monitors (by means of TMP) the dialyser behaviour curve during treatment, progressively adjusting Qi.
If we decide to graduate Qi manually, the monitor will not modify Qi, and we will have to do so when we detect an alarm or warning on the monitor when TMP increases. If we use the manual automatic or “alarm-free treatment”, we prescribe automatically adjusting Ht and TP values (since it is not possible to have the results of analysis for each session) to obtain a Qi value for manual prescription at the beginning of the session.
Other monitors (GAMBRO 200 Ultra-S® monitor) possess an ultracontrol module to adjust the replacement rate. The monitor automatically determines optimum TMP at the beginning of each session and, it adjusts it periodically every 60 minutes, based on the filtration fraction (Qb/Qi 30% ratio) and blood pressure on entry into the dialyser (system pressure), with the aim of achieving high UF volumes. This way, it is also possible to avoid having to increase TMP manually and, with it, the activation of alarms that interrupt dialysis.
In this study we have shown that automated manual prescription in postdilution OL-HDF is able to apply medical prescription (normally a Qi of about 25% of the Qb) with an individual intradialysis adaptation, according to blood viscosity and haemoconcentration during HDF. Furthermore, when applying an automated manual prescription, a similar replacement volume is obtained, with a reduction of 70% in the number of alarms, which means a considerable reduction of excess workload.
We conclude that prescription of automated manual Qi is a practical way of prescribing postdilution OL-HDF in which maximum efficacy and total replacement volume are achieved, with a significant reduction in the number of alarms during dialysis, which means an improvement in the patients’ clinical evolution, without any delays of the end-time.

Figure 1. Replacement volume (l) in the different study situations used.

Figure 3. Distribution of alarms according to the type of infusion used.

Figure 2. Dialysis dose in different types of infusion.

Figure 4. Total number of venous pressure (VP), transmembrane pressure (TMP) and haemoconcentration alarms.



